
Mechanics and Equipment
, The basic Swan-Ganz catheter is an invasive method of measuring pressure within the heart and the lungs. The triple lumen Swan-Ganz catheter is constructed of two open ended lumina plus a lumen connected to a balloon and a thermistor bead.We will now construct a Swan-Ganz catheter while describing the function of each component.
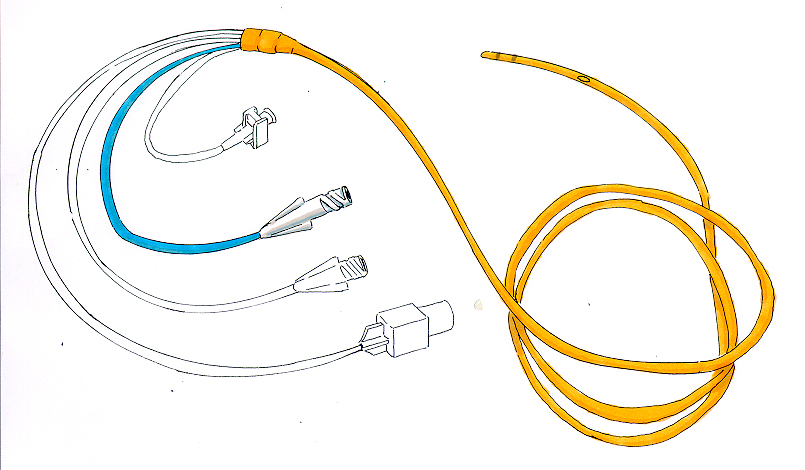
*Distal lumen of Swan-Ganz catheter.
The Distal Lumen is a fluid-filled line that transmits a wave of pressure from the tip of the catheter to the transducer. Remember that a transducer is a devise that converts one form of energy to another. The transducer converts the pressure signal to an electrical signal then sends it on to the monitor. The monitor amplifies the signal and displays digital readings and/or a waveform.
* The graphic above illustrates the Cardiac output computer that receives the electrical signal from the transducer. The transducer gets the pressure signal from blood moving in the pulmonary artery.
The catheter tip is 110 cm from the port and, if properly inserted, rests in a pulmonary arteriole. This port can help us measure problems that originate in the lungs, for example, pulmonary edema. Patency of the Distal lumen is achieved by maintaining a continuous flow of heparinized saline at a rate of 3cc an hour. The bag of Heparinized saline is placed under pressure using a modified blood pressure cuff (approximately 300 mm Hg), and infusion of solution is governed by a Sorenson Interflow

The diagram above shows a cannulated brachial artery but the pressurized bag of heparin, the transducer and the Sorenson intraflow devise are exactly the same setup used for a Swan-Ganz catheter.
When the Distal lumen is in a suitably small pulmonary arteriole, complete occlusion of the vessel is achieved by inflating the balloon with between 1/2 and 1 cc of air or CO2. We then take a reading known as PCWP (Pulmonary Capillary Wedge Pressure). This reflects what is going on on the left side of the heart. We immediately deflate the balloon once the reading is done to prevent pulmonary arteriolar necrosis.
*The graphic below shows the balloon fully inflated. The Syringe is attached to the red line.

The Proximal Port is connected to a Continuous Drip (usually D5W) to maintain Patency and/or administer drugs. The Lumen opens 30 cm from the catheter's port. If properly inserted, the proximal port is placed within the right atrium.
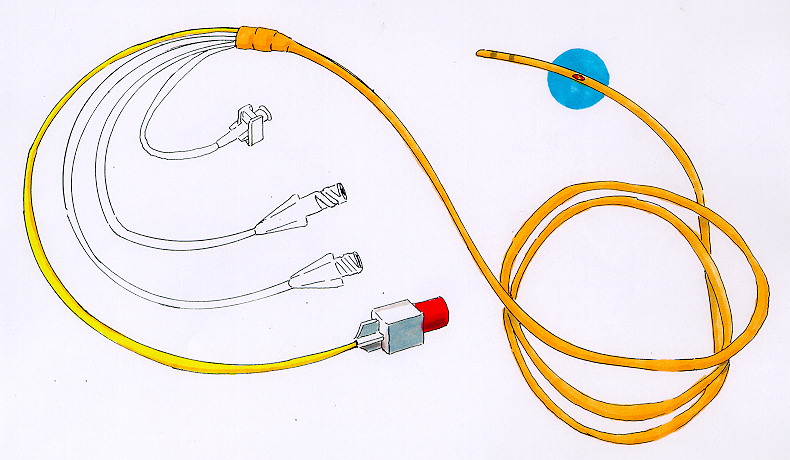
*The graphic below shows the CVP Port (blue) the opens into the Right Atrium.
Cardiac Output may be measured by injecting a bolus of saline, at a known temperature less than the body's, into the proximal lumen. A 10 cc syringe that has been iced is normally used. The thermistor bead, which is placed near the catheter tip, senses the resultant temperature of the blood as it passes by.
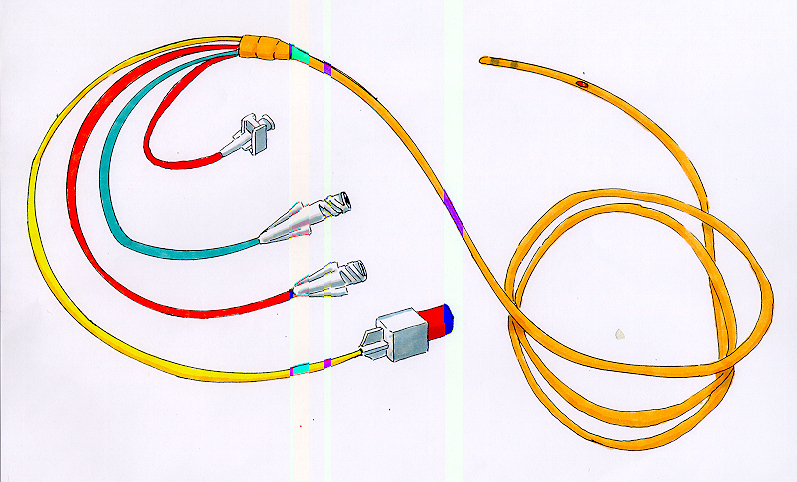
*The graphic below shows the Thermistor bead highlighted in blue. The yellow line with the red cap is attached to the transducer while changes the temperature of the blood into into an electrical signal that is amplified by the computer and readout as Cardiac Output in liters per minute.
The greater the Cardiac Output the more warm blood will be in the sample. With a smaller drop in blood temperature, this will be read as a greater Cardiac output. For example, if a normal adult Cardiac Output is 4-6 lpm, if the patient's CO is 5 lpm, the drop in blood temperature from 37 degrees Centigrade will be very small. This small drop in temperature will be read by the computer as a normal CO. Now suppose that the patient's CO is only 2 lpm, there will be a large drop in the blood's temperature, thus the thermistor bead will read this as a low CO.
*The graphic below shows the complete "bottom of the line" Swan-Ganz catheter with its four ports. This would be a good place to review to make sure you know the names of each port and what they do! You're allowed to go back and look at previous parts of this section.

*The above diagram demonstrates in more detail how the SvO2 is calculated. Fibroptic wires (both sending and receiving ) sit in the blood emitting light . The difference between the sending and receiving wavelengths is transmitted via the photodetector back to the computer to be amplified and transduced into a numerical value. The normal SvO2 is 70 %.

First, a review of the heart and its great vessels.
*The above graphic shows the Internal Jugular Vein (IVC)and the Subclavian Vein (SCV) draining into the Right Brachiocephalic Vein and then into the Superior Vena Cava (SVC). Normally the IVC and the SCV are first choice for the insertion of a Swan-Ganz catheter as they are a direct shot into the Right Atrium.
The Swan-Ganz catheter is inserted as a surgical procedure at the bedside using sterile technique.
We begin with a vein that is as close as possible to the right side of the Heart. The Internal Jugular Vein and the SubClavian Vein are the most likely first choices. If unsuccessful any peripheral vein may be chosen (i.e., the Basilic, the Cephalic or even the Femoral). In the case of the Internal Jugular or the SubClavian, the catheter advances into the right atrium via the Superior Vena Cava.
A Central Venous Pressure (CVP) reading may be taken at this point using the proximal port. The normal CVP tracing appears on the monitor as follows:
*Graphic of Right Atrial (CVP) Pressure. Normal 2-7 mm Hg
.The catheter is then advanced through the Tricupsid Valve and into the right ventricle. The waveform changes the instant the catheter moves through the Tricupsid Valve. Why? Because Pressure recorded within the Right Ventricle is dramatically higher then within the right atrium. Why?
Graphic of Right Ventricular Pressures. Normals: Systolic 15-28 mm Hg, Diastolic 0-8 mmHg.
The balloon is now partially inflated and allowed to sail into the outflow tract of the Right Ventricle along with the blood when the catheter passes through the Pulmonic Valve and into the Pulmonary Artery. The Pulmonary Vascular bed is not as flexible as the Right Ventricle, therefore Diastolic pressures are somewhat higher.

Graphic of Pulmonary Artery Pressure. Normal: Systolic 15-28 mm Hg, Diastolic 5-16 mm Hg, Mean 10-22 MM Hg.

The Dicrotic Notch is a significant feature of the PA tracing representing the closure of the aortic and pulmonic valves at the end of systole. Loss of this notch in a PA tracing indicates repositioning of the catheter may be necessary. Loss of the notch may also be from patient movement. More about this in a later section.
The balloon is now fully inflated and the catheter advanced into the pulmonary capillary bed. Advancement stops when the waveform changes, indicating that the balloon is wedged in a pulmonary arteriole.
When the balloon is fully wedged, the distal lumen is isolated from the influences of the right ventricle, thus it now becomes a window into the left ventricle. Each time the Mitral Valve opens there is a direct communication between the catheter tip and the Left Ventricle via the pulmonary capillary bed.
Graphic of Pa and PCWP. Normal Mean PCWP 6-15 Mm Hg
Note that the Diastolic and Systolic Wedge Pressure are so close that only a mean value is reported.
Once a wedge pressure is measured, the balloon is deflated to allow perfusion of the distal pulmonary arteriole, thus the PA waveform is restored.
Now, the completed series of waveforms
Waveform as catheter tip passes through RA, RV, PA, PCWP and PA with balloon deflated. This concludes the section on mechanics and equipment
*The above graphic illustrates the EKG tracing on the top line while the bottom line depicts the CVP, RV, PA and PCWP tracings as a Swan-Ganz catheter is placed.